If you have questions or want information not shown in this document/page, please use the main menu to check this website. Your answer may be within! If you would like to contact Natalaya Schleuter directly, please use Facebook Messenger
So much on this journey is unknown to you, for now – but soon you will be an expert. I remember standing alone in the hospital with a mask on my face, two hot salty waterfalls streaming down my cheeks and apologizing for crying because I wanted so badly to be strong. My little girl was exactly one week old and was surrounded by four people, the word “severe” being thrown around again and again, beating up my heart in ways I could never explain. Severe. I was beyond unprepared. I was postpartum. I was standing there all alone – thank you, covid. I wished I had a support group from the beginning, that I had a heartfelt letter from another mom (even one I didn’t know) telling me it would all be ok, and the many unknowns clarified.
So I took a few of my evenings, with my two little girls sleeping in their beds, to compile a list to support others.
It looks overwhelming, but the advice within is made to support you and comes from the bottom of my heart. It is based on scholarly articles, advice from other parents, and the professional opinions of top orthopedists. If you have questions, concerns, or difficulties on the journey, please feel welcome to reach out to me!
Please remember, we have all gone through similar steps of the journey, you are not the first, and you aren’t alone. Take things one day at a time, one hour at a time, and when things are truly overwhelming, five minutes at a time. Take lots of photos, give lots of cuddles, get them to laugh – be your baby’s rock and their number one advocate – be the voice they do not yet have. Trust your instincts, but be open to advice because we are also taking care to help others with our stories and experiences.
You’ve got this!
Created by Natalya Schluechter - mom of two wonderful girls
Course of the Ponseti Treatment (A Sample Schedule).
– Birth
– 1 Week Old – Cast #1
– 2 Weeks Old – Cast #2
– 3 Weeks Old – Cast #3
– 4 Weeks Old – Cast #4
– 5 Weeks Old – Cast #5
– 6 Weeks Old – Cast #6
– 7 Weeks Old Tenotomy + Tenotomy Cast (stays on for 3 weeks)
– 10 Weeks Old – Tenotomy Cast Removed, BnB Introduced
Bracing Begins!
– 23h wear for 3 months (first week of adjustment is usually very difficult)
– 4-6 Months Old – 23h wear Graduation! – reduction to 20 hours --child learning to sit/crawl
– 6-8 Months Old – 18h wear introduced --child learning to sit/crawl
– 8-10 Months Old – 16h wear introduced --child learning to pull up
– 10-12 Months Old - 14h wear introduced, - Child may be learning to take steps
– 1st Birthday – 12-14h wear until 5th birthday (stay closer to 14h) - Child learning to walk
The gradual reduction schedule allows your child to learn the skills all other children are learning, and they can also learn to do these things with the BnB on. They are not hindered in any way!
However, it is perfectly normal for a clubfoot child to be a couple months delayed with walking, though my daughter has been well ahead of schedule right now – she flipped back to tummy at 3.5 months and crawled one week before 6 months.
*Tenotomy.
90% of clubfoot children will have a tenotomy surgery (it isn’t full-on surgery!) – it is as simple as cutting a tongue tie and leaves a tiny scar on the back of the leg. The doctor uses a scalpel to make a small puncture in the back of the foot, cutting the Achilles tendon. The Achilles tendon is lengthened, thus improving flexibility of the ankle. No stitches are required. The final cast is then applied.
Tenotomy can be done either in the clinic with local anesthesia (much like a tooth cavity) or in the operating theater with general anesthesia. When worrying which is better, there are pros and cons to both. While Dr Ponseti performed tenotomies in the normal clinic room and the child could go home immediately, sometimes children can be quite active and today’s doctors are opting for the operating room – sterile conditions and a baby that is sedated and not kicking like crazy. We had partial sedation and it was very hard on her stomach – diarrhea for weeks, but I wouldn’t change how we did it.
– Take lots of photos between cast changes, especially the soles of the feet. Documenting whether your child had a crease at birth is important, because any doctor who may later say a foot is atypical when there was no crease at birth to begin with are suspect (a red flag). If your child is born with atypical feet, as my girl was – please consider taking the time to look for a doctor specialized in atypical/complex feet, there are very few in the world that are so skilled.
– Always take a photo of how the feet look when leaving the casting appointment in case the feet slip in the cast. Plus make sure to mark location of toes with the edge of the cast with a permanent marker.
– Starting casting early isn’t indicative of the best success. In fact, waiting one month can yield better results. But, starting early means being in BnB earlier, and getting through the 3 month 23-hour wear period faster, when baby isn’t as “strong” and “active”.
Helpful items for casting days.
– Castings typically take ~15 minutes for cast removal and ~15 minutes per leg, in my experience.
– Bottle of Milk
– Cherry-pit pillow to microwave & keep casts warm in the first 24 hours
– Extra Diaper
– Extra Onesie, castings can get wet!
– Pacifier
– Sugar Water is sometimes offered to calm the baby
– White Noise (my girl calms with it immediately, the doctors and nurses were impressed!)
Vaccinations.
– A baby in casts can be vaccinated. There’s no reason to hold off vaccinations, although waiting a few weeks usually isn't detrimental for most infants.
– Vaccinations can be done into the upper thigh or the arm.
Diaper Blowouts (oh no!).
– Long Panty Liners (prevention) Leg Warmers (prevention)
– Cut toes of sock and use like a leg warmer (prevention)
– Cotton Roll + Coban Roll (*after blowout* pad ½ into cast, secure w/ Coban) Cotton Roll + Medical Tape (*after blowout)
Baths in Clubfoot Casts (sponge baths).
– Babies are clean – they don’t run or jump or play in the dirt yet. The dirtiest they will get is inside the diaper, so a sponge bath is relatively simple.
– Wet a washcloth in warm water (I didn’t even use soap!), rinse, wipe down baby, repeat. Easy!
– Amazon Basics Washcloths Pack of 24 (inexpensive, easy to throw in the washing machine)
– Warm bucket of water
See examples of how to hold your baby while in casts as well as other helpful hints and ideas for casted babies on the Holding Baby with Casts page.
Sleep Sacks.
– Aden + Anais Dreamland Weighted GroBag
– Halo – top recommendation
– Merlin Sleepsuit
– Nested Bean
– Slumbersack (up to size 6-10 years!)
– Zipadee Zip
Bracing During Sickness .
You do not need to remove the brace during sickness.
It's a slippery slope if you imagine every sniffle or fever means the brace needs to be off.
You remove it for one night,
but the next night your child still has a fever,
so it’s one more night, and…
off we go taking the brace off regularly.
They are sick, they are fussy, they have a fever, and they are unhappy, but it's not about the brace, it's about the discomfort of being sick. The child does not think wearing the brace when sick is added discomfort, we think that as parents. They always wear the brace, they are used to that. They aren't used to being sick.
Removing the brace could actually cause more issues (i.e. rejection of the brace or relapse). We brace through fevers (39.2 (102.5) was the highest we had), diarrhea, vomiting, etc.
Sicknesses where brace removal may be needed (continue bracing unless truly severe discomfort):
Hand Foot & Mouth Disease or Chicken Pox
BnB (Boots and Bar) Brands (Foot Abduction Braces (FABs)).
The Foot Abduction Brace/Bar or commonly known as "BnB" (Boots and Bar) holds the corrected feet in place during a child’s growth, and more importantly, growth spurts (my girl’s foot grew half a centimeter in a week visibly!). If the boots aren’t put on correctly and very tightly, you are risking not only relapse, but also blisters and pressure sores.
Different Brands and Manufacturers of BnB and FAB Braces for Clubfoot.
The Bnb (Boots and Bar), FAB (Foot Abduction Brace/Bar), DBB (Dennis Brown Bar) is always the same basic design
- Shoes attached to a bar abducted and dorsiflexed for clubfoot bracing after correction with the Ponseti Method.
Mitchell Boots - Titled "AFO's" on the MD Orthopaedics website.
Ponseti Bar+ (340 grams for bar + size 00 boots; bar is adjustable, aluminum - Available through MDOrthopaedics.com
Dobbs Bar
Model SDCBMD (6months and older usually [because it is heavy])
Alfa Flex Bar + Comfoot Boots (Germany) we had it in the beginning & switched to Mitchell
C-Pro Direct BnB(static bars not adjustable, all bars should be sent with initial order - contact your orthotist if they don't give them all to you initially. New articulating sytem is adjustable)
Blisters/Pressure Sores.
**Blisters form due to friction – make those boots are tight so there is no movement inside!
**Creams before putting on socks. While a good intention, can cause blisters (exceptions: Foot Glide/Compeed Stick).
– DuoDerm – cut 1-2cm larger than the sore (round, no corners!), allow to fall off on its own
– FootGlide Anti-blister BalmTalc Baby Powder in Socks
– Moleskin - put a layer or two (or three) on the inner heel of the boots may help. (Moleskin does not by itself prevent blisters - only use if absolutely necessary and never use on baby's skin itself)
– Sheepskin from tandy leather – stitch to strap at a shoe repair shop
Pressure Saddles.
(use sparingly as they can potentially affect dorsiflexion due to their stiffness) USAEurope (Poland)
When used, the middle strap can be too loose, causing the foot not to be placed well in boot.
The pressure saddle is stiff and is placed on the dorsal side of the foot, exactly where the foot flexes up. When something is on the dorsal side, it limits the foot movement “up”.
Round cotton make-up sponges can be used as an alternative to pressure saddles. These are also helpful for when the foot is between holes as they can take up that extra bit of room until the foot grows a little.
Bunions.
Sometimes children will develop bunions from the boot buckle. You can take the boots to a shoe repair shop and have them stitch the buckles in lieu of the rivets. This is very uncommon.
Socks (for BnB).
I recommend having 6 pairs of any one size.
– Avoid thick/fuzzy socks - hinder getting heel flat, can cause extra sweating + athlete’s foot
– Choose lighter colors so you can see the heel more clearly in the hole
– Socks aren’t the most important aspect of successful BnB, properly tightening the boots is
– For more books and bar covers, and other cool stuff for clubfoot families: https://nosurgery4clubfoot.com/stuff
Walkers/Bouncers/Saucers/Pikler Triangle.
Many doctors say no to bouncers/saucers and even walkers because the foot can plantar-flex or the child uses their tippy toes rather than the full foot. In 2018, the American Academy of Pediatrics called for all infant walkers to be banned. The AAP says they don’t help children learn how to walk, and in contrast, can actually delay when a child starts to walk because the movements they use to move a walker around doesn’t translate to the movements needed to walk independently, and the children can’t see their feet and legs. The overall message from experts is that jumping devices are okay as long as they are not used for more than a short period of time (15 minutes) and they are freestanding, not attached to doorways.
In the grand scheme of things, 15 minutes is really not much time at all and can easily be filled by another activity.
Things to consider purchasing instead:
– Pikler Triangle with Ramp. Best if it is foldable and over 80 cm tall as it will grow with your child.
– Indoor Gym/Playground . We have one (photo) and are lucky to be using it with our second girl now – best 330 euro investment for what is going on 4 years of fun (especially in winter). We read under it, play camping, climb, jump, slide!
Baby Cranky All of the Sudden with BnB?.
You feel like your child is suddenly rejecting BnB completely, kicking their feet like crazy, crying, waking frequently or fighting sleep.
Check that the bar is the correct length, sometimes we completely forget to check bar width.
These items are best to be selected in-store whenever possible. Recommending which car seat would work is difficult as car seat brands vary internationally, as do international standards. Every car is different, one car seat could easily fit into a large car but would be pressed in a smaller car. And, if a family has several children, the fit in the entire back seat is called into question. Also, as outlined in the next section, only the first year of life is of true consideration, as is wearing BnB in the car seat.
Wearing BnB during car rides is a controversial topic in the clubfoot community. A lot of doctors are torn on whether to allow it on car rides – some say yes, others to keep boots on, others no. Why?
There are a few known cases when car accidents have caused broken legs due to baby wearing a brace in the car seat.
Rule of thumb can be: are the child’s feet touching the seat of the car?
It depends on your car travel timings and how your child behaves in the car.
Are you frequently on the road? – consider not risking it, take the bar off
For long stretches? – consider keeping it off
Just to the supermarket? – keep it on
Does your child take long naps in the car? It’s your risk. Remember, a child with their muscles at rest risks relapse, which is why we wear BnB during sleep.
Also, remember that during the first year you're bracing for long hours but after the first birthday this will mainly be night-time only with a long afternoon nap, so the consideration is really mostly for the first year of life regarding wearing the brace in the car.
Relapses and Bracing for Children Treated with Ponseti Method.
(approved by Dr Jose A Morcuende)
Relapses are a common occurrence among children with clubfoot up to the age of six years. The following is the rate of relapse for discontinuing brace-wearing at the age designated:
1st year 90%
2nd year 70-80%
3rd year 30-40%
4th year 10-15%
5th year+ ~6%
Severity of clubfoot deformity at birth is not a reliable indicator of the odds of relapse. Therefore almost all clubfoot patients are held to the same bracing protocols in order to provide them with the best protection against relapse.
– 23 hours for 3 months (typically begins at ~3 months of age)
– 20 hours for 2 months (typically begins at ~6 months of age)
– 18 hours for 2 months (typically begins at ~8 months of age)
– 16 hours for 2 months (typically begins at ~10 months of age)
– Graduation to 12-14 hours ~first birthday
Why gradual reduction?.
– Babies do not like sharp transitions or changes to routines. Dropping to naps/night time can lead to brace rejection and sleep problems.
– If for 3 months it was critical to brace 23h and not allow for more time without the brace, why is it suddenly allright to decrease to 12h?
– Because the relapse risk is at a staggering 90% in the first year.
– It allows for a good mix between time in the brace and active time without it.
Reduction of hours per Dr Morcuende (tied to nap time averages per month of age):
“I advise to use brace full time for 3 months, followed by 14-16 hours for 3 months. By this age (7-8 months old) the baby starts to sit and even crawl some, so it is best to let them develop and use the brace only at night for 12-14 hours. When they walk independently around 14 -16 months, they use it for 12 hours until 4-5 years old.”
Why is wearing BnB during naps important?
Babies fall asleep hard and deep very quickly. Deep sleep makes the whole body relax: it is not active – muscles, tendons and ligaments do not work because they are not set in motion by the brain. Due to “muscle memory” each relaxation of the foot during sleep requires the use of a brace, even when the child sleeps 10 minutes.
Relapse.
If your child relapses, the entire process of clubfoot management repeats – yes, imagine a few weeks of casting, possibly a repeat tenotomy and more long hours of bracing. This is why properly adhering to the BnB hours is important and especially going through gradual reduction in the first year, as it reduces the risk of relapse.
23-hour wear for a baby with gradual reduction in the first year is much easier to do than risking a relapse and the same for a toddler who has learned to walk.
100% parental adherence to bracing protocol does not mean your child will 100% not relapse, but it decreases the odds of relapse drastically.
BnB Angles (degrees of abduction).
– Corrected clubfoot: 60 - 70 degrees abduction
– Unaffected foot: 30 - 40 degrees
– (The last cast applied to a corrected clubfoot should have been rotated to 60 - 70 degrees unless complex)
Complex Clubfoot Angles (degrees of abduction).
If the child has been diagnosed with atypical (at birth) or complex (improper casting) clubfoot, the boot for the corrected clubfoot should be set to 20 - 30 degrees and worked up to 40 - 50 degrees. In general, BnB angles are to be set to the same angle as the final cast abduction.
These articles discuss abduction degrees and treatment of complex clubfoot in great detail, including the method for doing so, which differs from that of treating regular clubfoot:
"This type of clubfoot is difficult to treat and requires modification of standard Ponseti technique. Adduction of forefeet should not be corrected beyond 40 degrees to prevent hyperabduction at tarso-metatarsal joint."
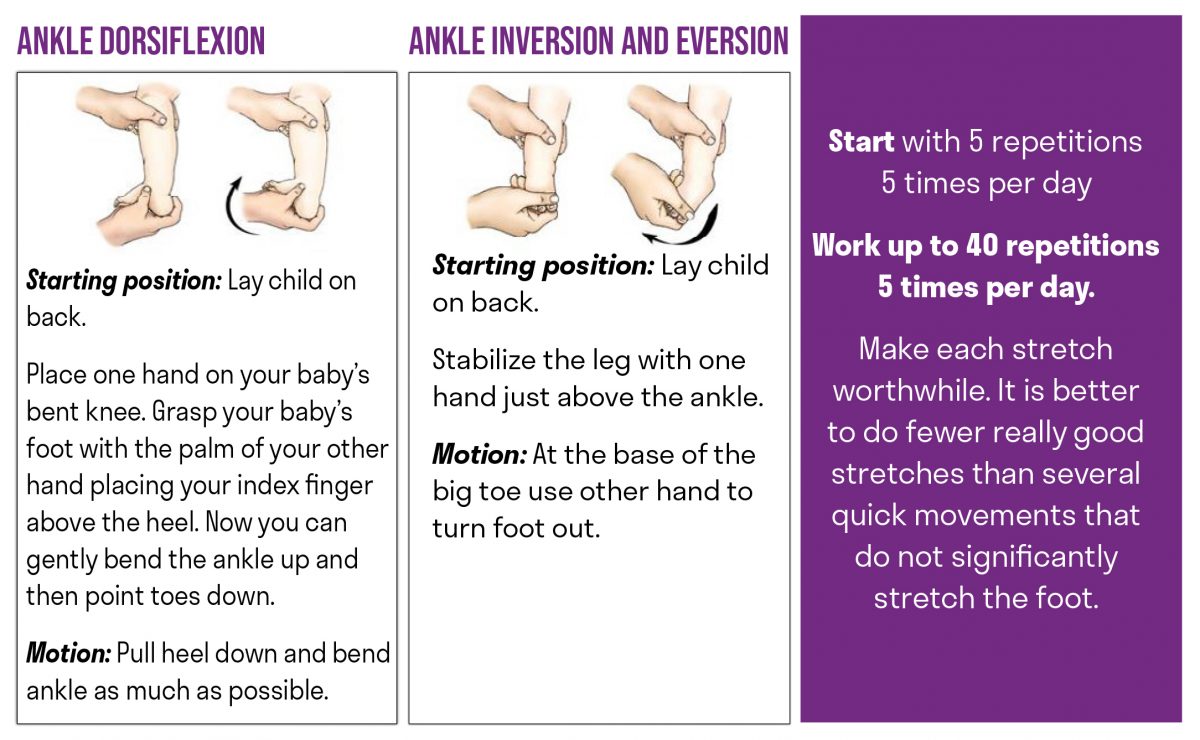
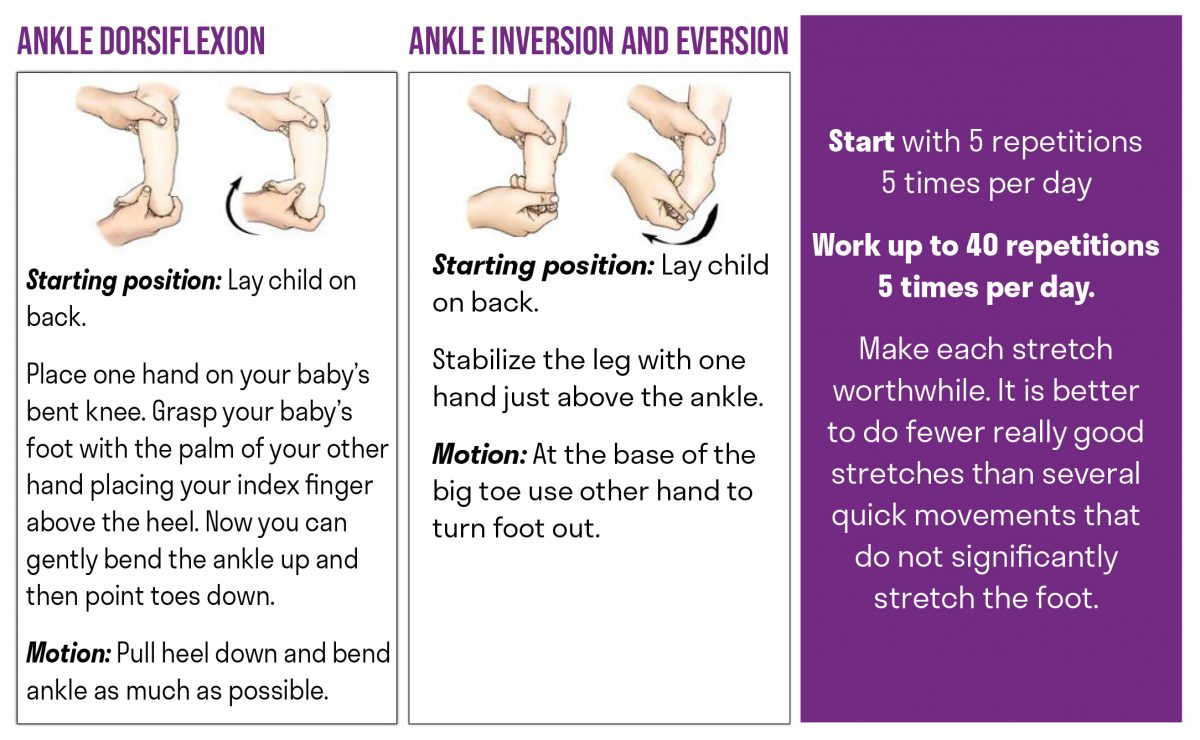
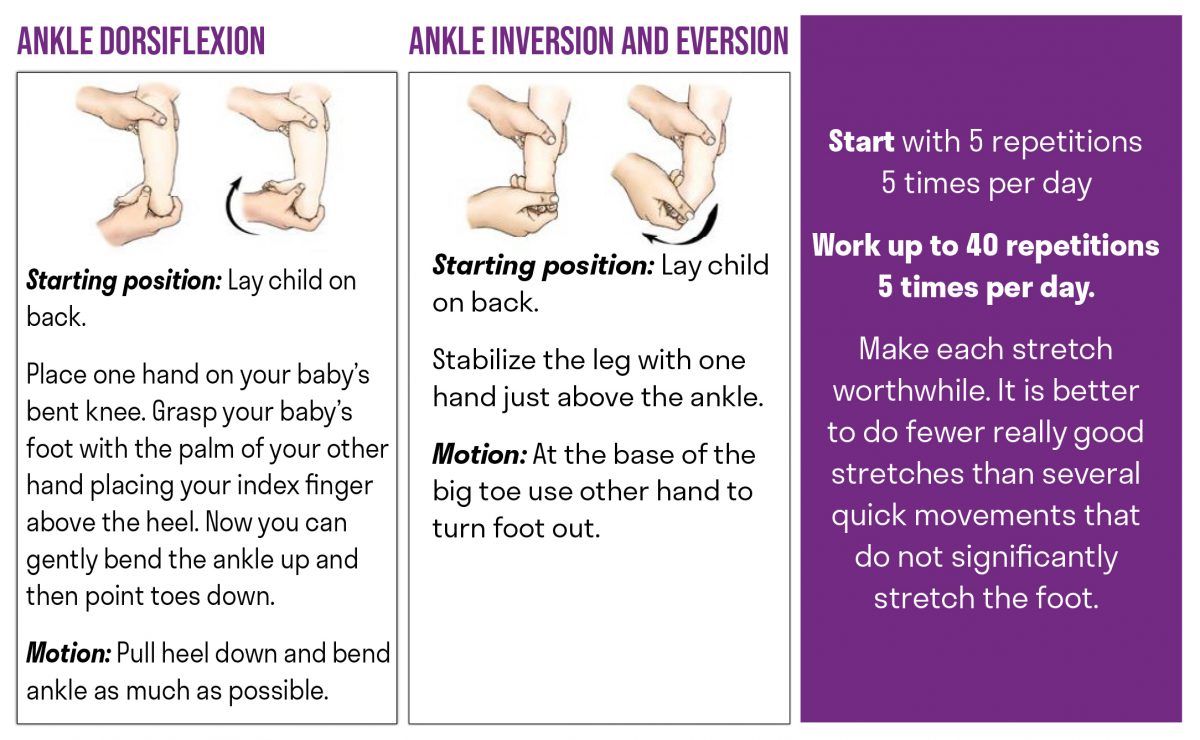
Following the traditional Ponseti method, stretches are not necessary – the child naturally stretches the foot through bracing, walking, playing and daily activities. Do choose floor play at home over a long walk in the stroller outside whenever possible to activate those muscles!
Of course, stretches can only positively impact your child, but they should be pleasant and not bring stress, discomfort, pain, or tears. Here are some links to stretching material:
Please send used medical equipment (boots and bars, pavlik harnesses, prosthesis...):
LIMB-art Ltd Nant-y-Lladron Bylchau Conwy LL16 5SN Wales United Kingdom
(Casting) Questions for Your Doctor.
credit: Kori Rush
Ask some seemingly hard questions. Don’t feel nervous about asking these things, and don’t worry about taking the doctor’s time. If they can’t answer these questions without much thought, there is a problem.
Ask about your doctor’s experience. How long have they been using the Ponseti Method? How long have they treated clubfoot, how many clubfeet have they successfully treated, who trained them and what had that training entailed. Ask if they were trained by Ponseti International or some other source, and who was that trainer trained by? You’re looking for someone in their background who was actually trained by a Ponseti Method expert.
Ask about casting material - should be plaster, unless they are amongst the elite skilled with fiberglass.
Ask how often their casts slip and what they do about it. Slipped casts are always the fault of the doctor, not an “active” child or the parent carrying the child a certain way, or sitting in a car seat. Slipped casts should be removed ASAP to avoid complex deformities that would require an elite set of hands to fix (we currently know of 15 doctors that skilled globally) (rocker bottom, midfoot deformity, etc). If you have even the thought that the cast has slipped, remove immediately.
Ask the average number of casts they use (5-7 is norm), when they take each cast off (should be weekly, except for tenotomy cast which is 3 weeks) and how it’s removed (should be right before the next cast, a few hours maximum, not the night before – as per Dr Dobbs the feet can stiffen quickly).
Ask which brace they prescribe and how that’s done (when are feet measured, who is the orthotist shop, etc). Ask for contact details in case adjustments are needed, or if something breaks.
Ask what their bracing schedule is (gradual reduction or sudden drop to 12hr? How many years?) You’re looking for gradual reduction during the first year, bracing for 5 years and not any less.
Most importantly, ask what is their overall success rate.
What is their ATTT (anterior tibialis tendon transfer rate)?
ATTT is a procedure used to treat recurrent clubfoot. You’re looking for percentages there. How many surgeries they do and when, at what age? (answer should be: after all casting and bracing options have been exhausted, only then is ATTT considered after age 4).
What is their approach for relapse? Casting/repeat tenotomy/23-h wear?
You need to find out what you want to hear from these questions. What relapse rate is ok with you? Do you agree that your doctor should be Ponseti trained, or is it ok that random people did the doctor’s training? Do you think plaster casts are essential? Are you concerned about modifications to the Ponseti Method such as bracing schedule modifications or do you want to follow all of the statistics/studies and really give the best chances for your child?
Knowing enough about what you are willing to accept helps when you formulate these questions and analyze the answers you’re given. Some deep research into the Ponseti Method might be helpful for your own comfort.
BnB Questions for Your Doctor.
– Best way to contact them (bruising, blisters, pressure sores, etc.)?
– What is the doctor’s on-call policy?
– Is there a doctor you can talk to on weekends/off hours and this doctor’s expertise?
– What will the reduction of hours look like (wear policy)? You want gradual reduction
– Should I remove the BnB for car rides?
– How long will this pair of boots last us until we need the next pair?
– How do I order the next pair of boots, how long does ordering take?
– How often should we have check-ups/meetings with you?
– Advice on walkers/gliders/bouncers?
RED FLAGS.
– Casting material should be plaster. Fiberglass, which sounds like “stronger” material, is not traditional for the Ponseti Method is incredibly difficult to work with. Fiberglass is less heavy and slips more often.
– Excessive casting. The Ponseti Method typically has 4-6 casts.
– Toes that overlap in the casts. If the doctor says this is “ok”, don’t be afraid to ask if the doctor’s own toes are currently overlapping in their shoes.
– Casts not bent to 90 degrees at the knee.
– Casts that are not reaching the upper thigh – half-leg casts are not ok.
– Cast removal should be maximum a couple hours before the next cast is placed, not the day/night before. “Feet tighten up quickly.” – Dr Dobbs.
– Curvature of the feet after casting. When looking at the bottom of the foot, the sides of the foot should be straight.
– Hyperextension of the big toe.
– Crease on bottom of the foot that was not present at birth signifies that a foot has been made complex. Complex feet should be handled by doctors skilled in such – there are only a handful of them in the world.
Casting Red Flags.
Feet slipping inside casts are always the fault of the doctor. This can cause complex feet. If a cast slips – remove the cast immediately. Don’t second guess this. No cast is better than a slipped cast!
Many doctors are blaming strong, willful or older babies on cast slips.
One cast slip here and there is ok, two or more are really big red flags.
– Feet that begin to have a crease on the sole that was not there at birth – your doctor is making the foot complex, which means it will be hard to fix this foot and you will need to find one of the very few doctors in the world who are able to fix complex feet.
– Feet can be “overcorrected” and look crooked and bent outward. This is not the same as abduction to 70 degrees which is also considered an "overcorrection". Get a second opinion immediately if baby's sole isn't straight on the outside.
– Crease on bottom of the foot that was not present at birth signifies that a foot has been made complex. Complex feet should be handled by doctors skilled in such – there are only a handful of them in the world.
BnB.
A sharp reduction of hours from 23 hour wear to 12 hour wear is not recommended for best success preventing relapse in the first year, and in subsequent years.
If the first 3 months of bracing at 23 hours is critical and we are warned just how critical it is, why is it ok to have a sharp drop in hours?
Babies are especially vulnerable to big changes in their life. For months they were used to wearing the brace for 23 hours and a severe shift away can be very shocking. This can lead to rejection of the brace.
Many parents are looking forward to bracing less, but this also increases risks. Just because some children were “just fine” dropping in hours and never relapsed doesn’t mean it will be the same for your child.
In the event of a relapse, being able to say “I did everything I could as a parent for my child” will eliminate a lot of potential guilt you may have over how you did things.
– Ending BnB before age 5. *See relapse rates on Page 7.
– Doctors who state that BnB makes any form of correction to the feet – it only maintains the correction.
– Doctors who state that BnB makes any form of correction to the feet – it only maintains the correction.
– Doctors using experimental braces. If you can, insist on proven BnBs, as outlined above.
– Doctors who have little or no concerns over open sores.
– Doctors who insist on 23 hour wear for the first year or until baby is pulling up. 3 months of 23 hour wear is all that is needed, followed by a gradual reduction of hours ending with 12-14 hours at the first birthday. This is then the amount of hours to be braced until 5 years of age, preferably staying closer to 14 hours and bracing during naps and sleep, when muscles are at rest and prone to relapse.
Find a Doctor
We can help you find the best Ponseti Method doctor for clubfoot treatment

{kind=link}
{kind=link}
{kind=link}